Home » Health News »
The secrets to self-confidence, according to cognitive science

In 2019, 7.2% of people in the European Union suffered from chronic depression. The human—and economic—cost of this illness is considerable, which is why the European Commission unveiled a €1.23 billion mental health strategy in June, to be achieved through 20 flagship initiatives.
Science shows that self-esteem plays a key role with certain mental disorders, particularly those of anxious and depressive nature.
Even today, however, the cognitive mechanisms underlying self-esteem remain mysterious. If we are to understand them, we need to start by asking ourselves a set of questions:
- How is self-esteem expressed?
- Why does it vary from one individual to another?
- How do psychiatric disorders and self-esteem interact?
Situated at the intersection of neuroscience, mathematical modeling and psychiatry, our research aims to answer these questions to better understand self-assessment, a critical aspect of human cognition.
Here’s what we’ve learned so far, and the main hypotheses we’re pursuing.
Self-esteem and motivation
Research in psychology shows that a high level of confidence in oneself and one’s abilities is associated with a greater sense of control over what happens to us, which may promote our ability to take on challenges. When the latter are met with success, our confidence may enjoy a boost, propelling us into a virtuous circle.
Conversely, if a person lacks confidence when embarking onto a project, they are more likely “not to believe in it,” and therefore to give up trying. The chances of success—and consequently the opportunities to positively reinforce their confidence—are then reduced.
But is it low self-esteem that leads to the onset of anxiety or depressive disorders, or the reverse?
To explore these questions, we need to look at how individuals assess their performance.
A wide range of confidence
Let us preface what follows by stating there is huge variability in self-assessment. For example, a depressed person may underestimate their ability to complete a task despite performing on a par with others, while a person suffering from cognitive problems (in the early stages of dementia, for example) may continue to trust their own abilities.
This variability, the origins of which are not fully known yet, takes two main forms.
- The degree to which the confidence judgments made by an individual enable them to discriminate between their own correct responses and their errors. For example, one can tend to be overconfident, but still be less so when one is wrong than when one is right. Conversely, one can be overconfident, but equally so, regardless of the correctness of one’s answer.
- The existence or not of a gap between subjective confidence and objective performance.
We’ve all noticed that some people underestimate themselves, while others overestimate themselves. On the other hand, some are “well calibrated”—they are able to show a high level of confidence when their objective performance is high, and a lower level when their performance is truly lower.
At the population level, a well-validated finding in behavioral psychology and economics is that we are (slightly) overconfident. A case where the numbers speak for themselves is that more than half of people think that they are better than average drivers or are more intelligent than the average.
Different levels of confidence
Scientists have long struggled to differentiate variations in confidence from those in other cognitive characteristics. The task is made all the more difficult by the fact that confidence is expressed at different hierarchical levels:
- Our confidence in a given decision (“I answered this question correctly”);
- Our confidence in a task (“I did pretty well in that exam”);
- Our confidence in a given cognitive domain (“I have a good memory”);
- …up to our self-confidence, which constitutes an overall level.
These distinctions are important: one can be confident of one’s ability to drive in bad weather (perceptual domain), while not being sure one can remember a list of things to do (memory domain).
Similarly, for certain types of exercise one may be able to “know when one knows and know when one doesn’t know,” whereas for others it may be trickier to distinguish one’s mistakes from one’s successes.
Two main hypotheses
There are currently two main coexisting hypotheses about the mechanisms underlying confidence judgments.
One is that there is a central self-assessment mechanism that estimates confidence in any given response or task. This mechanism would be the same across different domains, such as memory, language or reasoning. In this case, actions designed to improve the accuracy of self-assessment should aim to “re-educate” or “train” this very central judgment capacity, independently of the task at hand. The benefits would then become widespread.
The second hypothesis postulates that our confidence judgments are not the result of a central self-assessment mechanism, but are intimately linked to each domain. According to this hypothesis, any action designed to improve the accuracy of self-assessment should therefore target the relevant task or domain.
Both hypotheses remain hotly debated. Whether at the behavioral or neurological level, research results tend to indicate that the reality is probably somewhere in between. There is no single centralized mechanism (which would probably not confer enough flexibility), but neither is there a specific mechanism for each domain—that would be too “costly” for the brain to maintain.
Mental health profiles in the population
Another hurdle in the study of self-assessment and confidence is that the current classification of psychiatric disorders is in the process of being rethought.
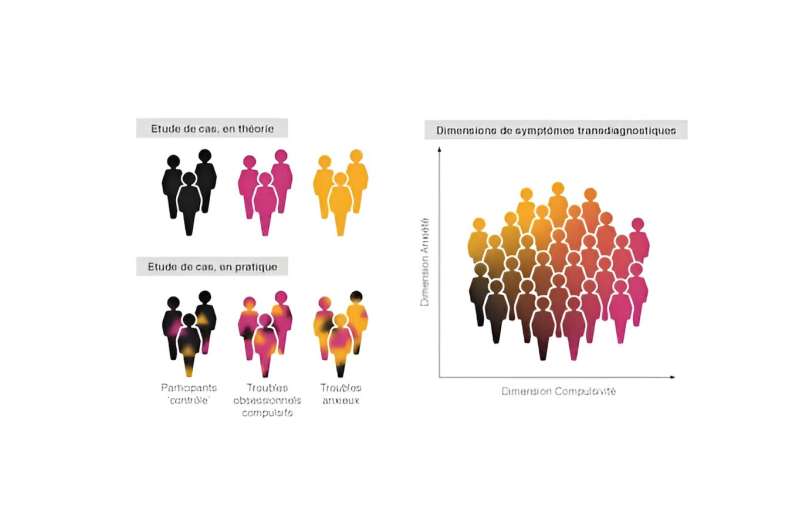
This is particularly true of the idea that a symptom is equivalent to an illness. Anxiety, for example, is not a diagnostic symptom of a single psychiatric disorder—one can be anxious when suffering from depression, a borderline personality disorder, and so on. Conversely, an illness does not necessarily limit itself to a single symptom. Take the case of an obsessive-compulsive disorder (OCD), where some patients experience high levels of anxiety, whereas others do not. Yet their diagnosis is the same.
This makes it challenging to reliably predict which treatment option would be most effective for a given patient. Indeed, while the traditional classification is clinically relevant, it does not always directly match the neurobiology of psychiatric disorders.
Complementary to this traditional viewpoint, the so-called dimensional approach focuses on the heterogeneity and variability in underlying symptoms, which may be common to several illnesses. This alternative classification is understood as transdiagnostic, one that works through traditional diagnostic categories.
Math can help to better capture mental health symptoms
Traditionally, psychologists and doctors have tended to diagnose mental health disorders by relying on patients’ reports. The latter can enlighten either by expressing themselves directly on the couch or by answering specializing questionnaires, including questions such as:
“Do you find it difficult to make decisions?” or “Do you sometimes feel so anxious that you find it hard to breathe?”
Using machine learning, researchers attempted to group the symptoms in such a way as to identify common points to different pathologies, rather than studying each illness separately. Once groupings of symptoms common to several diseases had been established, experimental techniques could be used to better grasp the biological, cognitive or behavioral mechanisms involved.
In the case of OCD, machine learning methods could potentially identify subgroups—for example, an “anxiety” subgroup. The hope is that this will make it possible to offer treatments or psychotherapeutic methods that are better suited to each individual. Indeed, a person with anxious OCD may not respond in the same way to a given treatment as a person with OCD where anxiety is less pronounced.
In the general population
The idea is that mental health symptoms naturally fluctuate, both in patients and in the entire population. This is true even with those who have not been diagnosed with a psychiatric disorder—we are all to some degree more or less anxious, more or less impulsive, more or less obsessive, and so on.
Applying machine learning methods on volunteers, we found that people with more compulsive and intrusive thinking symptoms generally reported higher confidence, but had a less accurate self-assessment. This pattern could be related psychological effects such as a tendency to jump to conclusions.
Moreover, people with more marked anxious and depressive symptoms were found to have lower confidence in their decisions, but a more accurate self-assessment—which may be related to the notion of “depressive realism”. However, these results seem to depend on the domain in which we are evaluating our confidence (for example, memory, sport, etc.).
A better understanding of how confidence judgments are formed could help us determine why self-assessment varies from one person to another. It could also help us gain awareness of the gap that can exist between our performance and our perception of it.
Provided by
The Conversation
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Source: Read Full Article

