Home » Health News »
Low-risk, long-term cancer survivors more likely to die of non-cancer causes, study shows

Advances in early detection and treatment have vastly improved the long-term survival of people diagnosed with cancer.
This increasing population of long-term cancer survivors, many of whom are over age 65, has created unique challenges for U.S. oncologists and primary care providers in determining how best to coordinate and prioritize patient care. As the country’s population continues to age and more people experience higher risks for cancer—as well as other age-related health problems—these challenges are expected to grow.
A new study led by Yale University researchers provides information that could help. The researchers examined the cancer- and non-cancer-related mortality rates of long-term adult cancer survivors to better understand and quantify their associated health risks. The findings could help reduce large-scale care inefficiencies and improve the quality of care for long-term cancer survivors, who have unique cancer and non-cancer health needs. The findings are published in the journal JAMA Network Open.
“The population is aging, and people who have cancer are living longer,” said Yale School of Public Health Associate Professor Michaela Dinan, co-leader of the Cancer Prevention and Control Research Program at the Yale Comprehensive Cancer Center and the study’s senior author. “What we’re trying to do is make sure that this population is receiving efficient care and also the best quality of care.”
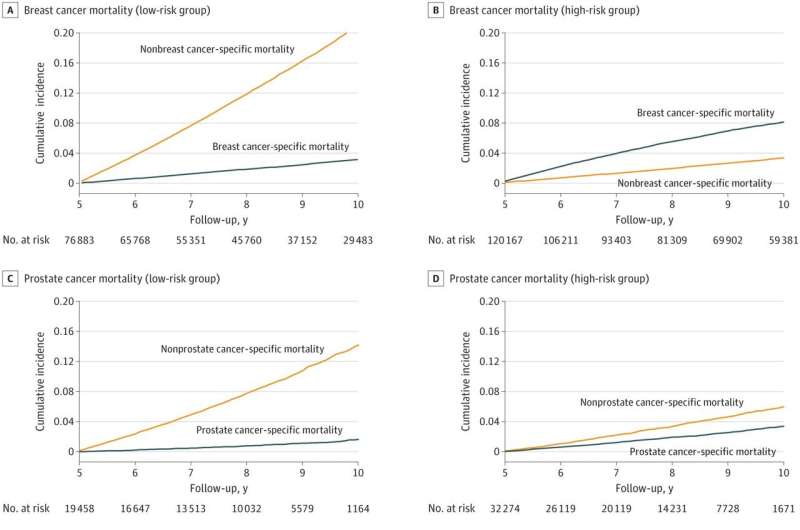
One of the study’s key findings was that low-risk, long-term cancer survivors are at least three times and up to nine times more likely to die of a cause other than their initial cancer. For the study, long-term cancer survivors were defined as adults who live at least five years past diagnosis.
The study looked at 628,000 patients who were diagnosed with breast, prostate, or colorectal cancer between January 1, 2003, and December 31, 2014, received treatment, and were alive five years after diagnosis. The patients were broken into three risk categories—low, intermediate, and high—based on their risk of dying from their diagnosed cancer.
For breast and colorectal cancer, low-risk patients were 65 or older and stage I, high-risk patients were younger than 65 and stages II or III, and intermediate-risk patients were the remainder. The categories were similar for prostate cancer, except the Gleason score was used instead of cancer stage.
The researchers looked at whether the patients died from their diagnosed cancer or something else, including a new cancer type, within 10 years of their diagnosis.
High-risk patients for all cancers studied except prostate were more likely to die of their initial cancer, the study found. But low-risk patients were at least three times more likely to die of something else. Low-risk breast cancer patients were nearly seven times more likely to die of a cause other than their initial breast cancer and low-risk prostate cancer patients were nine times more likely to die of something other than their initial cancer diagnosis. Low-risk colon and rectal cancer patients were seven and three times more likely to die of causes other than their initial cancer, respectively, the study found.
The researchers found that heart disease made up one-fourth of all deaths not caused by the original cancer. Alzheimer’s disease, chronic obstructive pulmonary disease, and cerebrovascular disease were the next most common causes of death.
The findings offer important insight for the care of long-term cancer survivors, Dinan said. A common model for cancer patients in the U.S. is that care is transferred from a primary care provider to an oncologist after diagnosis, Dinan explained. The oncologist manages all care and the former primary care provider often has little input. This may continue indefinitely, she said. But the long-term feasibility of this model, and whether it provides patients the best care, is a growing concern, she said.
Given the country’s population is aging and that many cancers begin when people are in their early or mid-60s, there eventually won’t be enough oncologists, Dinan noted. Long-term survivors also have more complex health needs than the general population, and not all of those needs are related to their cancer. They have a higher risk for developing a new cancer, becoming seriously depressed, developing cardiovascular disease, or becoming frail with age, Dinan said.
“Their original breast or prostate or colon or rectal cancer doctor is not the appropriate person to be monitoring them for those health conditions,” she said.
Risk-stratified care models could be a useful strategy for better allocating care between oncologists and primary care physicians. The American Cancer Society, the American Society of Clinical Oncology, and the National Cancer Institute view these models as an important area for research.
The current study is a first step in a larger American Cancer Society grant that Dinan and her research team received to develop risk-prediction algorithms for informing long-term survivor care. Dinan is currently studying risk factors for these survivors developing other diseases, such as the patient’s cancer stage at diagnosis and whether the patient received radiation or chemotherapy. Her goal is to predict and then validate what makes patients a high, medium, or intermediate risk for different health conditions.
Patients and their physicians could eventually use this information in conversations about care, she said. A low-risk breast cancer patient also at low risk for cardiovascular disease might be best served by being transferred back to her primary care provider, while one at high risk for cardiovascular disease might need to see a cardiologist promptly.
“Personalized risk stratification is feasible, and it can help prioritize goals of survivor care management,” she said.
More information:
Madhav KC et al, Relative Burden of Cancer and Noncancer Mortality Among Long-Term Survivors of Breast, Prostate, and Colorectal Cancer in the US, JAMA Network Open (2023). DOI: 10.1001/jamanetworkopen.2023.23115
Journal information:
JAMA Network Open
Source: Read Full Article
-
 You Can Now Smell Like Your (and Gigi Hadid's) Favorite Teen Face Scrub
You Can Now Smell Like Your (and Gigi Hadid's) Favorite Teen Face Scrub
-
 Low amount of caffeine intake during pregnancy may help reduce gestational diabetes risk
Low amount of caffeine intake during pregnancy may help reduce gestational diabetes risk
-
 'Approved' or 'authorized'? When it comes to COVID-19 vaccines, words matter.
'Approved' or 'authorized'? When it comes to COVID-19 vaccines, words matter.
-
 Remote ischemic preconditioning can amplify the protection against heart attack, stroke
Remote ischemic preconditioning can amplify the protection against heart attack, stroke